In a recent study posted to the medRxiv* preprint server, researchers developed a coronavirus disease (COVID-19) model-inference system in South Africa to determine transmission dynamics and immune evasion associated with severe acute respiratory syndrome-associated coronavirus disease (SARS-CoV-2) Omicron variant.
 Study: SARS-CoV-2 transmission dynamics in South Africa and epidemiological characteristics of the Omicron variant. Image Credit: Shutterstock
Study: SARS-CoV-2 transmission dynamics in South Africa and epidemiological characteristics of the Omicron variant. Image Credit: Shutterstock
Immunity and transmissibility associated with Omicron
After the initial cases of the SARS-CoV-2 Omicron variant were reported in South Africa in late November 2021, the number of Omicron cases increased rapidly in several provinces of South Africa as well as across the world.
Previous laboratory studies indicated that the Omicron variant could erode adaptive immunity, evident from the reduced Omicron neutralizing ability of convalescent COVID-19 patients and vaccine recipients. In addition, several preliminary studies showed that the replication rate of Omicron is higher compared to the SARS-CoV-2 Delta variant.
These shreds of evidence indicate increased immune erosion and transmission dynamics with the Omicron variant.
About the study
In the present study, the authors reconstructed SARS-CoV-2 transmission dynamics in nine provinces of South Africa using a model-inference system and determined the immune erosion and transmissibility of the novel SARS-CoV-2 Omicron variant.
The model-inference system used in this study was based on the authors’ previous study on immune erosion and transmissibility associated with SARS-CoV-2 variants of concerns (VOCs) like Alpha, Beta, Gamma, and Delta.
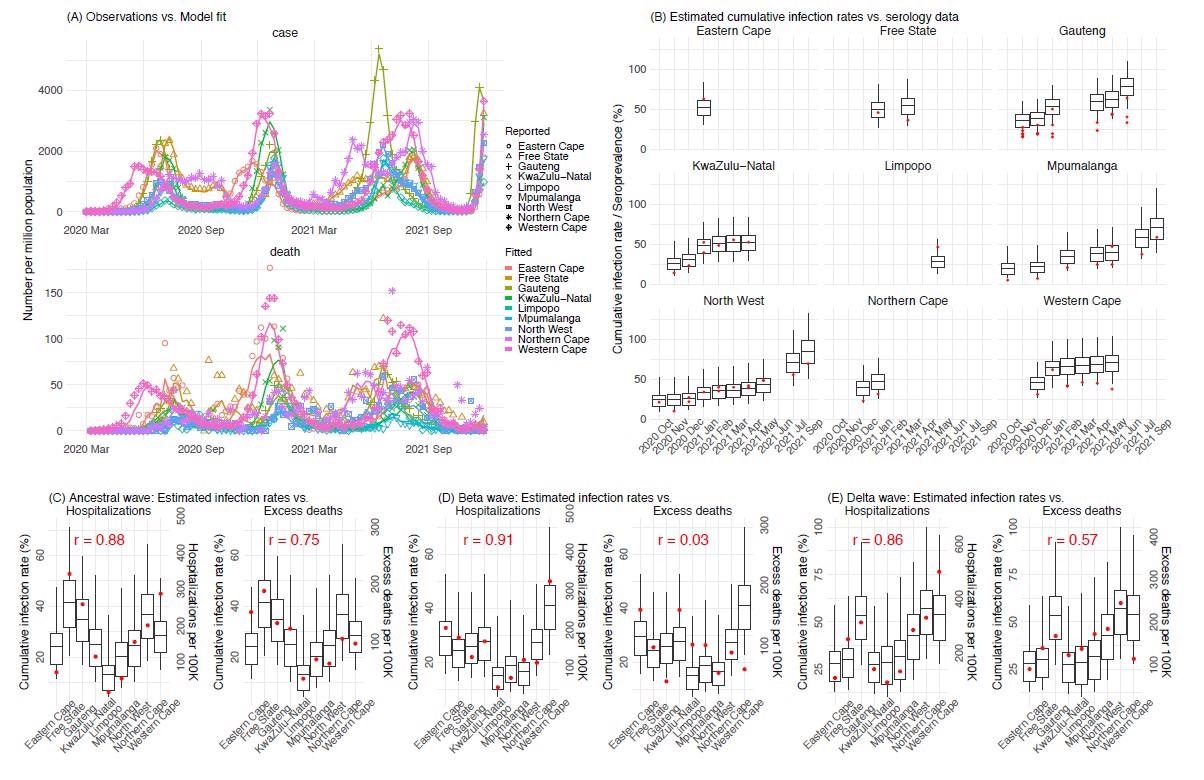
Pandemic dynamics in South Africa, model-fit and validation using independent data. (A) Pandemic dynamics in each of the nine provinces (see legend); dots depict reported weekly numbers of cases and deaths; lines show model mean estimates (in the same color). For validation, model estimated infection rates are compared to seroprevalence measures over time from multiple sero-surveys summarized in ref 1 (B), COVID-related hospitalizations (left panel) and age-adjusted excess mortality (right panel) during the Ancestral (C), Beta (D), and Delta (E) waves. Boxplots depict the estimated distribution for each province (middle bar = mean; edges = 50% CrIs) and whiskers (95% CrIs). Red dots show corresponding measurements. Correlation (r) between model estimated cumulative infection rate and cumulative hospitalization or age-adjusted excess mortality (C-E) for each wave is shown in each plot. Note that hospitalization data begin from 6/6/20 and excess mortality data begin from 5/3/20 and thus are incomplete for the Ancestral wave.
Weekly cases and mortality data accounting for the infection seasonality, under-detection of infection, vaccination, and implemented nonpharmaceutical interventions (NPIs) were used in the model. Databases such as coronavirus COVID-19 (2019-nCoV) Data Repository for South Africa (COVID19ZA), National Oceanic and Atmospheric Administration (NOAA), and Google Community Mobility Reports were used for data collection.
The model-inference estimates were validated using serology data from South African COVID-19 Modelling Consortium, COVID-19-associated hospital admission data collected from COVID19ZA, and the ancestral and Delta wave associated age-adjusted excess mortality data collected from the South African Medical Research Council (SAMRC). The key model-inference estimates were developed from the Gauteng province data as it had the earliest surge of SARS-CoV-2 Omicron variant, and the majority of their population were previously infected by SARS-CoV-2 ancestral, Beta, or Delta variants.
Results
After accounting for the infection seasonality, under-detection of infection, vaccination, and NPIs, the results indicated that SARS-CoV-2 infected most South Africans before the Omicron wave.
The model-estimated cumulative infection rates were higher than the province-based seroprevalence measures obtained at various time points. They correlated well with the COVID-19-associated hospitalization data from the ancestral SARS-CoV-2, Beta, and Delta variants across the nine South African provinces. The estimated infection numbers also correlated with the age-adjusted excess mortality associated with the SARS-COV-2 ancestral and Delta wave; however, they did not correlate with the SARS-COV-2 Beta wave.
Apart from the Gauteng province, high cumulative infection rates during the first three COVID-19 waves were estimated from Western Cape and Northern Cape provinces. The estimated average cumulative COVID-19 infection rates varied from 58% of the population in Limpopo to 126% in the Northern Cape provinces.
The Beta variant was 38.5% more transmissible compared to ancestral SARS-CoV-2 and associated with 72.1% immune erosion in ancestral SARS-CoV-2-infected individuals. In comparison, the Delta variant was 38.3% more transmissible compared to ancestral SARS-CoV-2 and associated with 32.5% immune erosion in ancestral SARS-CoV-2, Beta variant-infected individuals, or vaccine recipients.
Based on the data from the Gauteng province alone, the Omicron variant transmissibility compared to SARS-CoV-2 ancestral and Delta variant were 100.3% and 36.5%, respectively. Moreover, the Omicron variant was associated with a decrease of 63.7% of population immunity accumulated from previous SARS-CoV-2 infections and vaccinations. From the Gauteng, Northwest, and Western Cape province data, the transmissibility of the Omicron variant was 92.2% compared to ancestral SARS-CoV-2 and led to 55% immune erosion in previously infected and vaccinated individuals.
Conclusions
The researchers developed a comprehensive model-inference system for SARS-CoV-2 and estimated the transmissibility and immune erosion associated with the Omicron variant. According to the study, there was a high rate of immune erosion and transmissibility associated with Omicron among the convalescent COVID-19 patients and vaccine recipients.
This study indicates the increased need for vaccination and booster vaccines as well as the establishment of safe and effective therapeutics for populations worldwide. Furthermore, the study results aligned with the previous preliminary and laboratory study reports associated with Omicron. Hence, these findings help contextualize and interpret the transmission dynamics of Omicron outside South Africa.
*Important notice
medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
- SARS-CoV-2 transmission dynamics in South Africa and epidemiological characteristics of the Omicron variant, Wan Yang, Jeffrey Shaman, medRxiv, 2021, doi: https://doi.org/10.1101/2021.12.19.21268073, https://www.medrxiv.org/content/10.1101/2021.12.19.21268073v1
Posted in: Medical Science News | Medical Research News | Disease/Infection News
Tags: Coronavirus, Coronavirus Disease COVID-19, Hospital, immunity, Laboratory, Medical Research, Mortality, Pandemic, Research, Respiratory, SARS, SARS-CoV-2, Serology, Severe Acute Respiratory, Severe Acute Respiratory Syndrome, Syndrome, Therapeutics, Vaccine

Written by
Shanet Susan Alex
Shanet Susan Alex, a medical writer, based in Kerala, India, is a Doctor of Pharmacy graduate from Kerala University of Health Sciences. Her academic background is in clinical pharmacy and research, and she is passionate about medical writing. Shanet has published papers in the International Journal of Medical Science and Current Research (IJMSCR), the International Journal of Pharmacy (IJP), and the International Journal of Medical Science and Applied Research (IJMSAR). Apart from work, she enjoys listening to music and watching movies.
Source: Read Full Article


