
Oral cancer is a common cancer that affects the head and neck region. Around 50% of oral cancer patients do not survive for more than five years, even after treatment, as many patients seek medical help only during the late stages of the disease. By the time the patients seek help, the cancer may require advanced treatment, and may even have spread to other areas.
Oral cancer often develops from white patches clinically known as oral leukoplakia (OL) and oral lichenoid mucositis (OLM). These white patches may appear long before a diagnosis of oral cancer, and their early detection and continuous monitoring are crucial to prevent the development of cancer. However, it is sometimes challenging to predict which OL/OLM lesions will develop into oral cancers as the global risk rates of progression from OL/OLM to cancer vary from 0.4 to 40.8%.
Routine visitation and multiple biopsies are often scheduled during OL/OLM surveillance. In addition, patient monitoring may continue for many years leading to fatigue and lack of compliance with hospital appointments. Therefore, it will be better to determine the risk of cancer development in these patients on an individual basis to allow health professionals to use this information to formulate specific treatment and follow-up schedules for each patient.
Researchers from the Faculty of Dentistry and the Li Ka Shing Faculty of Medicine, the University of Hong Kong (HKU); Department of Pathology, Queen Mary Hospital, HK; and College of Medicine and Dentistry, James Cook University, Queensland have collaborated to develop a web platform that can be applied to automatically generate an individualized prediction of the risk of oral cancer occurrence in those with OL or OLM for up to 20 years following diagnosis.
The results are published in the journal Cancers in an article entitled “Deep learning predicts the malignant-transformation-free survival of oral potentially malignant disorders.”
The freely available web tool, based on the artificial intelligence algorithm “DeepSurv,” was trained and tested with data from patients with OL/OLM treated in Hong Kong (716 patients) and Newcastle Upon Tyne, UK (382 patients). As the patients have already been under review for many years, their true risk levels were already known, and the study showed that the artificial intelligent model was able to accurately predict their risk levels at different time points during their follow-up hospital visits.
The DeepSurv algorithm was selected due to its superior performance for the use of routine demographic, clinical, pathological, and treatment information of these patients for cancer risk prediction following a series of validation exercises.
On a validation subset of the Hong Kong cohort, “DeepSurv” was able to predict the correct cancer risk level for 95% of the cases. This was according to an integrated Brier score of 0.04, with a score below 0.25 generally depicting a tool that may be useful in real-world applications.
The algorithm is further able to generate correct risk levels for 82% of the patients in the British cohort which suggests its utility in other populations as well.
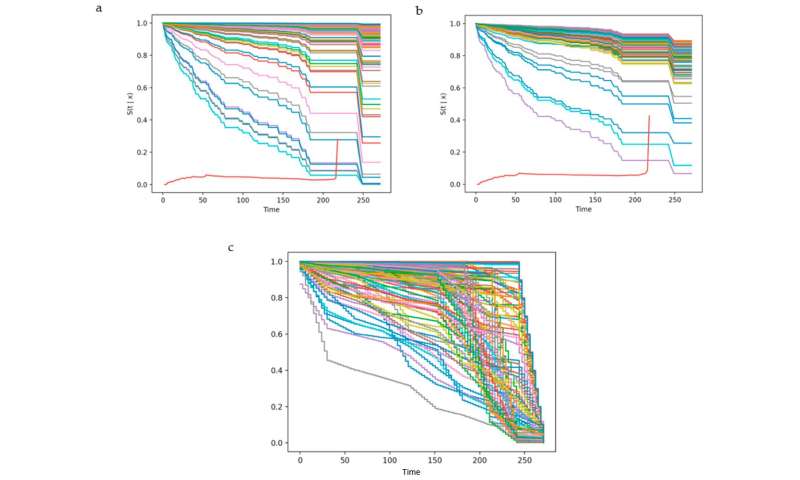
The interactive web tool requires 26 pieces of information on the demography, clinical and pathological description of the disease, and treatment received by the OL/OLM patient. The predicted output from the web tool includes a curve from which the different risk levels (vertical axis) can be visualized at each time point (horizontal axis). These predicted risk levels have been shown to be accurate up to 17 years from the time that the information was entered.
This will assist health professionals in the selection and prioritization of treatment strategies and close-monitoring schedules for high-risk patients, especially in resource-limited hospitals. Ultimately, this is expected to improve on the currently available methods of prevention and early diagnosis of oral cancer.
The prediction curve may also be used for individual cancer risk estimation and inform health professionals when to commence very close monitoring of patients when a certain risk level is reached.
For OL/OLM patients, risk awareness may motivate them to regularly attend routine follow-up visits and allow them to make informed decisions when providing consent for biopsy when required.
Of note, the predicted risk curve may change with varying input data such as smoking and alcohol drinking status, parts of the mouth that are affected, treatment received, lesion recurrence, and the severity of epithelial dysplasia during treatment monitoring.
“While the web tool has been found promising based on our validation exercises, users should know that it is still primarily a research-based tool and requires further prospective optimization,” said Dr. Richard Su, Clinical Associate Professor in Oral and Maxillofacial Surgery (OMFS), Faculty of Dentistry, HKU, who led the study.
Source: Read Full Article


